Everything about ovulation
What is ovulation?
Ovulation, also called egg release, is the release of a fertilizable egg cell from a mature ovarian follicle, known as the Graafian follicle. It is the culminating moment of each menstrual cycle, without which the conception of new life is impossible.
Preparation for ovulation
For ovulation to occur, the entire process of growth and maturation of an ovarian follicle must take place. From the several hundred thousand primordial follicles that are permanently present in a woman’s ovaries (and even in a girl’s ovaries before birth), a group of growing follicles begins to develop. Over time, one of them becomes dominant and outpaces the others in development. When the dominant follicle reaches a diameter of about 10 mm, it continues to grow at an average rate of about 2 mm per day (for 6-7 days). When it reaches a size of at least 20-26 mm, it is considered a mature Graafian follicle, ready to rupture.
The process of follicular growth and maturation is stimulated by follicle-stimulating hormone FSH (follitropin), which is secreted into the bloodstream by the pituitary gland.
How ovulation occurs
The maturing ovarian follicles produce estrogens, whose levels in the blood gradually increase, reaching a maximum about 36 hours before ovulation. At this point, the pituitary gland releases the amount of luteinizing hormone LH necessary to trigger ovulation. The LH surge precedes ovulation by about 24-36 hours, and its peak occurs about 12-24 hours beforehand.
Ovulation predictor kits available in pharmacies work on this very principle – they help detect the LH surge. The most favorable time to try to conceive is therefore the 2-3 days following the detection of the LH surge.
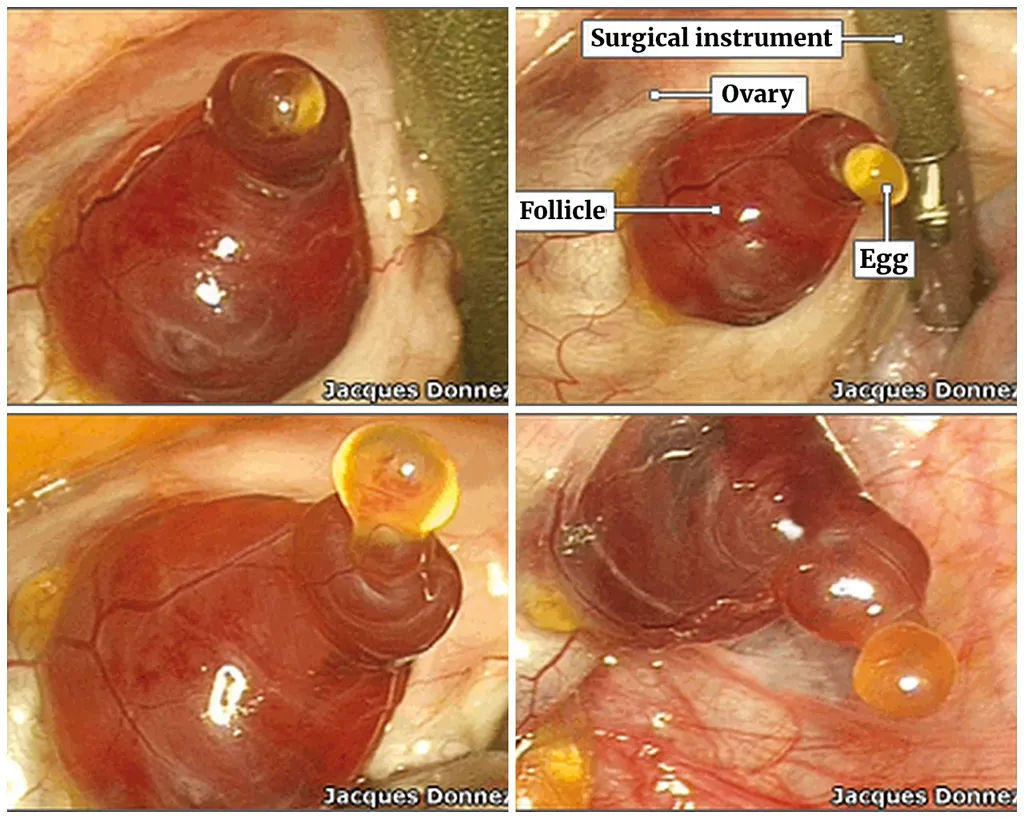
And this is what the moment of ovulation looks like, recorded during a hysterectomy procedure:
After ovulation, LH stimulates the cells of the corpus luteum formed from the ruptured follicle to produce progesterone, which prevents another ovulation from occurring in the same menstrual cycle.
The period from ovulation until the next menstruation, known as the luteal phase, may last from 11 to 16 days (and is relatively constant in a given woman). A shortened luteal phase may indicate an infertile cycle, while a prolonged one may suggest the onset of pregnancy.
Signs of ovulation
The rising level of LH in the blood stimulates the follicular cells to produce estrogens. The increasing concentration of estrogens causes several changes that are easy to observe:
- Softening, opening, and elevation of the cervix.
- Changes in cervical mucus produced in the cervical crypts that favor sperm survival: it becomes more fluid and diluted, creates a sensation of wetness and slipperiness, and becomes stretchy and transparent.
- Ovulation usually occurs on the so-called peak day of cervical mucus (about 38%), but it may also occur up to three days before or three days after the peak day [1].
- Typically, shortly after ovulation, a rise in basal body temperature to the higher temperature level is observed.
- Around ovulation, some women experience ovulatory pain (mittelschmerz) or increased libido, but these are secondary signs and do not precisely indicate the day of ovulation.
The period of optimal fertility (the so-called fertile window) covers the six days ending on the day of ovulation. The highest chance of conception occurs with intercourse two days before ovulation, but the exact moment of ovulation (which usually lasts about 15 minutes) is difficult to determine precisely at home. The only definitive confirmation that ovulation has occurred is the visualization of the released egg during a surgical procedure, ultrasound monitoring of the cycle, or… pregnancy 😉
When does ovulation occur for you?
If you observe your menstrual cycle, you should have no difficulty identifying this time:
- the days closest to ovulation are the day of the “mucus peak” and the following day, as well as the first day of the temperature rise and the day preceding that rise;
- confirmation that ovulation has taken place is a sustained rise in basal body temperature to the so-called higher level lasting for three days (which indicates a normal, fertile, biphasic cycle).
Ovulation disorders
Ovulation requires a strong surge in luteinizing hormone (LH). Without this peak, the Graafian follicle will not rupture, even if it has reached a considerable size. Likewise, if the process of follicular maturation is disturbed at the stage of the dominant follicle (for example, by stress or illness), this may lead to delayed ovulation or even to the regression of the dominant follicle. Preparation for ovulation is a process that is very sensitive to any disturbances, and therefore the egg may fail to be released from a mature follicle despite the occurrence of an LH surge. Several ovulatory disorders have also been described in the literature [3]:
- Luteinized Unruptured Follicle (LUF) – a Graafian follicle that does not release the egg but transforms into a normally functioning corpus luteum (Ober, 1957; Marik and Hulka, 1978).
- Ovum Retention – the Graafian follicle ruptures, but the egg remains trapped in the follicular wall and becomes enclosed within the forming corpus luteum (Craft, 1980; Stanger and Yovich, 1984).
- Empty Follicle Syndrome – a situation in which a follicle that is mature and ready to rupture contains no egg or cumulus oophorus (Rauscher and Ulm, 1963; Hilgers, 1989 and 1992; Coulam, 1986; Tsuiki, 1988).
How is ovulation blocked in women using hormonal contraception?
Hormonal contraception was originally designed to prevent ovulation and thereby prevent pregnancy. High doses of synthetic hormones (estrogens and progestogens) are intended to suppress the secretion of the natural hormones LH and FSH by the pituitary gland, thus creating a kind of “hormonal prosthesis” in place of the natural cycle of hormonal changes.
The first contraceptive pills introduced in 1960 contained very high concentrations of synthetic hormones and did indeed block ovulation, but they also caused numerous dangerous side effects, some of them even life‑threatening. To this day, manufacturers have been working to gradually reduce hormone doses in contraceptive preparations, yet adverse effects remain significant.
Unfortunately, many studies show that hormonal contraceptives do not always prevent ovulation. With combined oral contraceptives, ovulation may still occur in about 2-5% of cases. Even less effective in suppressing ovulation are progestogen-only pills (so-called “mini-pills”), with ovulation occurring in as many as 10-40% of cycles [4]. In such situations, the remaining contraceptive mechanisms are expected to operate, primarily the effects that impair the endometrium, making it unsuitable for implantation of a human embryo, and those that slow down tubal transport.
Based on:
[1] W.M. Moore, “Ovulation symptoms and avoidance of conception”, The Lancet, p. 588, March 11, 1972; and T.W. Hilgers et al., “The Peak Symptom and Estimated Time of Ovulation”, Obstetrics & Gynecology, 52(5), pp. 575–582, November 1978.
[2] J.B. Stanford, G.L. White Jr., H. Hatasaka, “Timing Intercourse to Achieve Pregnancy: Current Evidence”, Obstetrics & Gynecology, No. 6, Vol. 100, pp. 1333–1341, 2002.
[3] J. Rötzer and E. Rötzer, “My Cycle and Me: From Puberty to the Premenopausal Years”, INER, Warsaw, 2007.
[4] D.A. Grimes, A.J. Godwin, A. Rubin, “Ovulation and Follicular Development Associated with Low-Dose Oral Contraceptives: A Randomized Controlled Trial”, Obstetrics & Gynecology, Vol. 83, pp. 29–34, 1994.