Menopause – when a woman’s fertility comes to an end….

There is a period in a woman’s life that is associated with particular concerns and is often perceived by many women, to some extent, as a loss of femininity. Menopause. It is preceded by a time of major changes – above all hormonal ones (a decline in both estrogen and progesterone), and consequently also emotional and physiological changes. Once these take place, a new chapter in a woman’s life begins—and what it will be like depends largely on us. Let us therefore learn a little more to prepare for these changes.
When can you expect menopause to occur? What determines the timing of menopause?
With age, a woman’s fertility decreases significantly, menstrual cycles become irregular, ovulation occurs less and less often, and eventually menstruation ceases altogether. This process is individual for every woman, but it usually unfolds over several years preceding the last menstrual period.
In Poland, the average age at which menopause occurs is 50.1 years (natural median) [1]. In a study conducted at the Institute of Anthropology in Poznań in 2001, a sample of 4,354 women aged 35–65 was analyzed (women using synthetic hormones were excluded). In this study, menopause was defined as the last menstrual period confirmed by 12 months of amenorrhea (absence of menstruation).
It should also be remembered that menopause may occur as early as age 35 (early menopause) or after the age of 55 (late menopause).
Several factors have been identified as having a direct influence on the age at which menopause occurs: the age at first menstruation, the length of menstrual cycles, and coexisting factors such as the duration of breastfeeding, as well as the age at first and last pregnancy.
The age at which a woman has her first period (menarche) is strongly correlated with the age at which menopause occurs. The earlier a woman begins menstruating, the earlier she will usually enter menopause. Thus, if the first period appeared before the age of 12, the average age of menopause is 49.32 years. Menarche between the ages of 12 and 14 corresponds to an average menopausal age of 49.72 years. If the first period occurred after the age of 15, the average age of menopause is 50.18 years.
The length of the menstrual cycle is also positively correlated with the age at menopause. The longer the cycles, the later menopause tends to occur. With cycles shorter than 28 days, the average age of menopause is 47.51 years. For cycles lasting 28–32 days, the average age is 49.32 years, while for cycles longer than 32 days it is 51.35 years.
The duration of breastfeeding and a woman’s age at her first and last pregnancy are factors that correlate with the above and intensify their effects. They do not directly determine the age at menopause, but they strengthen the influence of the direct factors. Thus, a longer period of lactation may be associated with a later onset of menopause. The younger a woman is at her first pregnancy, the earlier menopause may occur.
The number of pregnancies, irregularity of menstruation, and marital status do not have a significant direct effect on the age at menopause. However, some researchers (e.g., McKinley [2], Stanford [3], Jaszman, Leidy Sievert [4]) have proposed a link between menopausal age and marital status, comparing married women with divorced and unmarried women. Their findings suggest that a later onset of menopause in women may be associated with the influence of pheromones in marriages and relationships in which a man is constantly present in the household.
Other factors that may accelerate the onset of menopause include:
- environmental and ethnic factors (e.g., African women tend to experience menopause earlier, Japanese women the latest);
- smoking;
- loss of an ovary at a young age;
- ovarian hyperstimulation (excessive pharmacological stimulation of ovulation);
- hereditary factors and genes;
- alcoholism and drug abuse;
- lifestyle and chronic stress;
- chemotherapy, diabetes, thyroid disorders;
- being a twin (about 50% of twins experience menopause around the age of 40).
Menopause may potentially be delayed by avoiding certain dietary substances, by using hormone replacement therapy (although some studies indicate the opposite trend [5]), and, of course, by genetic factors.
How can you recognize that you are entering the premenopausal period?
The climacteric process begins gradually already after the age of 35, but the first more noticeable symptoms usually appear after the age of 40. You may observe:
- the occurrence of irregular cycles: alternating longer and shorter cycles with typical ones; fluctuations in length of at least 7 days over a period of at least 10 months and more frequently;
- heavier or prolonged menstrual bleeding;
- the appearance of mid-cycle (peri-ovulatory) bleeding and breakthrough bleeding;
- the occurrence of single-phase cycles or cycles with weak temperature rises;
- shortening of the post-ovulatory phase (decrease in progesterone levels);
- ovulatory disturbances and lengthening of the pre-ovulatory phase;
- breast tenderness and changes (mastalgia, mastodynia);
- persistent dryness in the vaginal vestibule, disappearance of cervical mucus.
Hormonal changes in the premenopausal period include:
- an increase in FSH;
- disappearance of LH pulsatility;
- loss of ovarian follicles and a decrease in ovarian inhibin levels;
- a slight increase in estradiol (E2);
- a decrease in progesterone levels.
In the postmenopausal period one can observe:
- high levels of FSH and LH;
- low levels of estradiol (E2);
- low levels of progesterone;
- lower levels of androgens (androstenedione, testosterone, DHEA, DHEAS).
Can anything be done to prolong fertility and delay the onset of menopause?
Very good results in improving reduced fertility caused by luteal insufficiency (too low progesterone levels in the post-ovulatory phase) can be achieved with a three-month course of chaste tree (Vitex agnus-castus). It is also worth remembering to supplement magnesium.
Helpful in strengthening fertility signs and normalizing the menstrual cycle are plant oils, especially evening primrose oil (also used for PMS and migraines) and flaxseed oil, as well as fish oils, e.g., cod liver oil.
To improve the quality of cervical mucus, vitamin E with selenium, zinc with vitamin A, or vitamin B6 may be used under medical supervision.
It is also advisable to include so-called plant estrogens (phytoestrogens) in the diet, such as soy, flaxseed, sesame, potatoes, wheat, and apples.
What symptoms and complaints can you expect during this period, and how can you cope with them?
In 70–80% of women, symptoms related to estrogen deficiency occur. The duration of these symptoms varies greatly among individuals and may last from 2 to even 15 years.
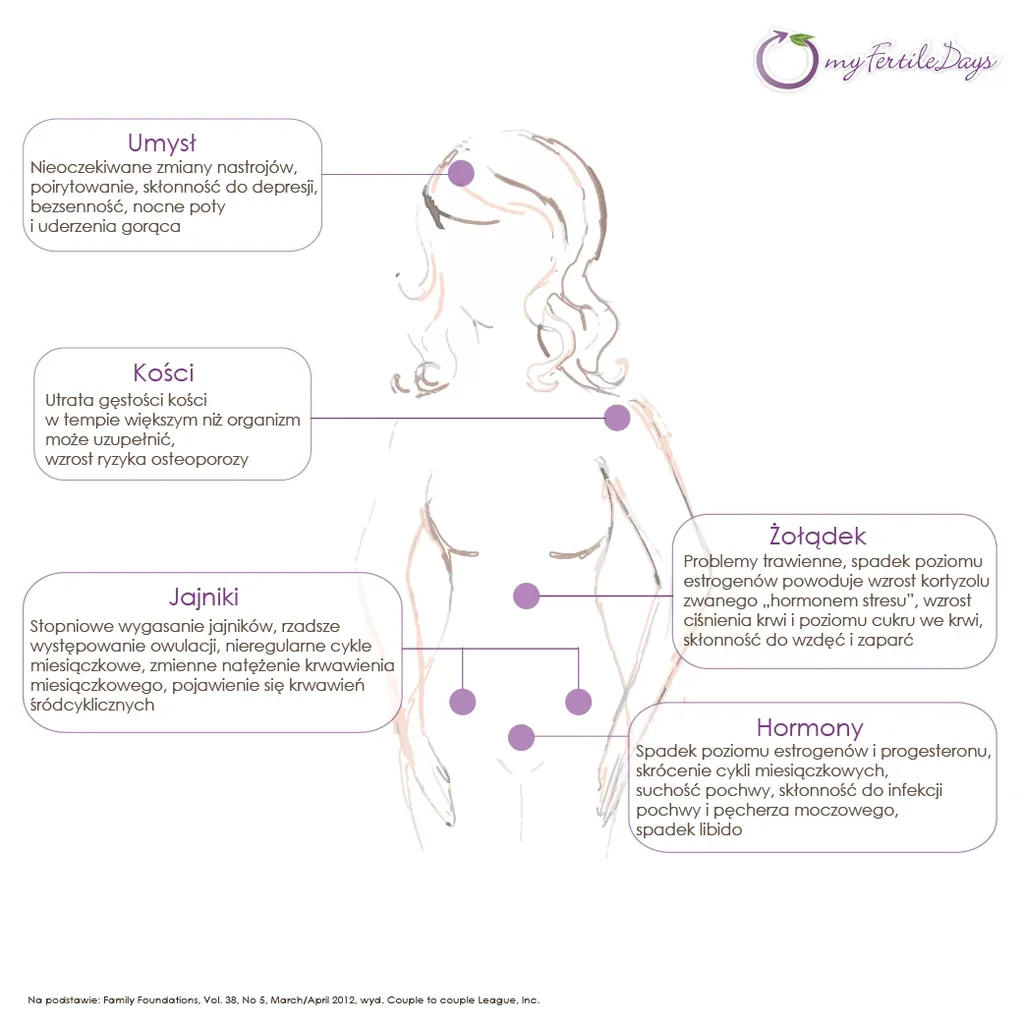
Menopausal symptoms may include:
- Vasomotor symptoms – hot flashes, profuse sweating, night sweats (which may also accompany conditions such as diabetes, pancreatic or thyroid disease, or chronic stress).
- Somatic symptoms – headaches, dizziness, memory problems, sleep disturbances, palpitations, weight gain, constipation
- Psychological symptoms – irritability, nervousness, tearfulness, depression, chronic fatigue, decreased libido.
- Physical symptoms – vaginal atrophy, vaginal dryness, bleeding, skin changes in the genital area, stress urinary incontinence, recurrent urethral and bladder infections (other contributing factors include childbirth, pelvic surgery, trauma, obesity, excessive physical exertion, hyperestrogenism, and congenital factors), and postmenopausal osteoporosis (additional risk factors include smoking, alcohol, coffee, excessive protein intake, low calcium and vitamin D3 intake, low body weight, and low physical activity).
Dietary recommendations to alleviate menopausal (climacteric) symptoms:
- avoid animal fats;
- increase the intake of plant oils (olive oil, evening primrose oil, fish oils);
- limit carbohydrates;
- include phytoestrogens (especially flaxseed oil, seed oils such as sunflower, whole-grain products, barley, oats, rye, legumes, red fruits, carrots, and of course soy products in moderate amounts); an Asian-style diet;
- vitamins: B6, B12, E + C, D3;
- folic acid;
- calcium supplements;
- use vitamin–mineral complexes specifically designed for women in premenopause and menopause.
In conditions such as mastodynia (marked breast tenderness), menstrual disorders due to corpus luteum insufficiency, chronic adnexitis, vaginal and bladder infections, uterine bleeding, and also in slowing the growth of fibroids, encouraging (and well-documented) effects are obtained with herbal preparations such as: chaste tree (Vitex agnus-castus), gypsywort (Lycopus europaeus), as well as bearberry, willow bark, chamomile, St. John’s wort, and calendula [6].
Moderate but regular physical activity is also highly beneficial, such as walking, Nordic walking, running, jogging, aerobics, yoga, etc.
Doctors quite often propose hormone replacement therapy (HRT) to relieve vasomotor and atrophic symptoms, and mainly to prevent osteoporosis. It is worth knowing, however, that for it to be effective it should be started about 10 years before menopause. Remember that these are synthetic hormones, so one should carefully consider whether the benefits outweigh the possible serious side effects, such as: worsening hypertension, thrombosis, venous disease, gallstones, weight gain, mastalgia, migraines, nausea, bloating, bleeding, and breast cancer. Some components of HRT are also suspected of increasing the risk of Alzheimer’s disease, heart disease, and stroke.
Contraindications to HRT include:
- liver disease,
- thromboembolic disorders,
- heart disease,
- history of stroke,
- breast cancer,
- endometrial cancer,
- vaginal bleeding of unknown origin,
- congenital lipid metabolism disorders.
There is a saying: “You work for your menopause all your life” – and it is very true. Diet plays a crucial role both in the age at which menopause occurs and in the intensity of its symptoms. Emotional factors are also extremely important: support from loved ones, self-acceptance, social engagement, maintaining relationships, taking on new challenges, having absorbing hobbies, or simply organizing daily work and activities well. All of this builds self-esteem and life satisfaction and helps not to focus excessively on the inconveniences of the menopausal period.
Based on:
[1] Maria Kaczmarek, Anita Szwed, “Age at menopause and reproductive determinants in Polish women”, Institute of Anthropology, Adam Mickiewicz University, Poznań. Przegląd Antropologiczny, Vol. 64, 57–72, 2001.
[2] McKinley S.M., Jefferys M., Thompson B., “An investigation of the age at menopause”, Journal of Biosocial Science, Vol. 4, 161–173, 1972.
[3] Stanford J.L., Hartage P., Brinton L.A., Hoover R.N., Brookmeyer R., “Factors influencing the age at natural menopause”, Journal of Chronic Diseases, Vol. 40, 995–1002, 1987.
[4] Leidy Sievert L., Waddlf D., Canali C., “Marital status and age at natural menopause; considering pheromonal influence”, American Journal of Human Biology, Vol. 13, 479–486, 2001.
“Menopause as a measure of population health. An Overview”, American Journal of Human Biology, Vol. 13, 429–434, 2001.
[5] Gold E.B., Bromberger J., Crawford S., “Factors associated with age at natural menopause in a multiethnic sample of midlife women”, American Journal of Epidemiology, Vol. 153, 865–874, 2001.
[6] W. Kapczyński, "Phytotherapy in gynecology and obstetrics", Fundamenty Rodziny, Vol. 49.