For the new mom: recognizing fertile days in the postpartum period.

Shortly after childbirth, significant hormonal changes occur in a woman’s body, profoundly affecting her mood and emotions. The level of endorphins, which play a role in inducing feelings of euphoria and relieving pain, decreases. With the expulsion of the placenta, the levels of sex hormones – estrogens and progesterone – also drop, which may lead to worsening of mood, persistent fatigue, or sometimes a state of apathy. At the same time, the level of prolactin, often referred to as the “motherhood hormone,” increases. Prolactin is responsible for milk production and inhibits the secretion of follicle-stimulating hormone (FSH), thereby preventing the growth and maturation of ovarian follicles containing an egg.
The return of fertility in the postpartum period depends mainly on high levels of prolactin, which are produced during lactation, but it is also influenced by lifestyle, stress levels, and a woman’s fertility status before pregnancy and childbirth.
To identify the days of fertility and natural periods of infertility effectively, you should start your self-observations as soon as possible to define the parameters typical for your menstrual cycle again.
- Carrying out your daily observations will allow you to get to know your body again, control your fertility and identify the fertile and infertile days properly.
- After the cessation of bleeding you should start your temperature measurements and observation of the mucus features to determine the basic model of infertility for you (or the presence of a constant secretion).
- After 12 weeks (or 6 at the partly breastfeeding), and before the first postpartum period, you should apply the Peak Rule, which allows you to determine the phase of infertility from the evening of the fourth day after peak symptoms of cervical mucus or cervix.
- The measurement of basal body temperature (BBT) helps determine whether the occurring bleeding is a menstrual period (which must be preceded by at least three days of high temperature phase) or it occurs in the periovulatory phase, indicating fertile days.
You should begin observations after childbirth once puerperal bleeding has stopped. Measure your temperature as often as possible immediately after waking to determine whether a high-temperature phase occurs before the first menstrual period. It may also happen that mid-cycle bleeding occurs during the low-temperature phase. Remember that getting up at night to feed your baby does not invalidate the temperature measurement.
You can also use the following tips:
- try to rest for at least one hour before measuring the temperature,
- ask your partner to look after your child for a while,
- set the alarm clock just before the time your child usually wakes up,
- measure your temperature while feeding your baby.
The temperature chart during the breastfeeding period is very characteristic – it is unsettled, with noticeable fluctuations in temperature. However, just before the first postpartum ovulation and the appearance of fertile cervical mucus, the chart typically becomes calmer and more stable.
After childbirth, it is important to relearn how to recognize the signals your body sends, as they differ from those you were accustomed to before pregnancy. These differences are especially noticeable during cervical self-examination, as the cervix may remain slightly open after birth. There may also be changes in basal body temperature levels in both the lower and higher temperature phases. However, the most commonly observed change is in the pattern of cervical mucus secretion.
If, after the cessation of bleeding after childbirth and the disappearance of any puerperal droppings, you don’t observe any presence of the mucus, then after the end of postpartum infertility – 6 weeks (no or partial breastfeeding) or 12 weeks (exclusive breastfeeding), such observations will also mean infertility. The appearance of any mucus will mean days of possible fertility.
However, if after puerperal bleeding has ceased, you observe a continuous presence of a certain type of cervical mucus – even beyond the postpartum infertility period (6 or 12 weeks) – the same symptom may indicate infertility, and only a change in the quality of the secretion signals days of possible fertility. In cases of constant secretion or a prolonged mucus phase, magnesium supplementation may be helpful.
Extending the intervals between feedings or switching to partial breastfeeding may lead to prolonged phases with mucus symptoms, which can make interpretation much more difficult. In such cases, cervical self-examination – which can be performed from the eighth week after childbirth – may be helpful.
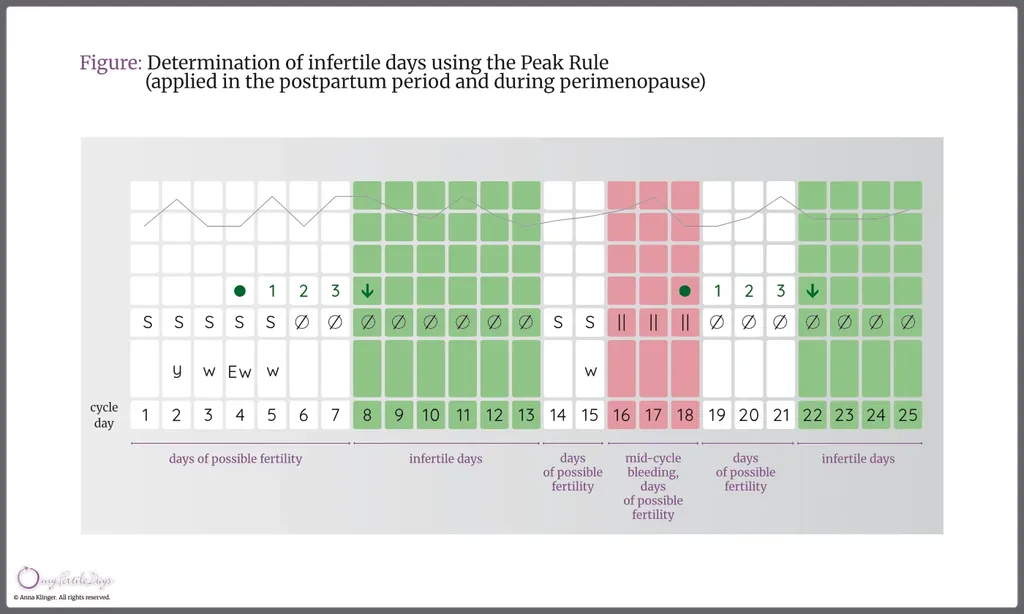
After the end of the period of infertility – 6 weeks (partial breastfeeding or lack thereof) or 12 weeks (full breastfeeding), and before the occurrence of menstruation – you should use the Peak Rule, which says:
- you can determine infertile days from the evening of the fourth day after the mucus peak, provided there has been no temperature rise and no additional signs of fertility have been observed;
- bleeding that is not preceded by a high-temperature phase (mid-cycle) is considered a mucus-related symptom, and its last day should be marked as the mucus peak. If, immediately after the bleeding, any signs of fertility are observed, the last day of the mucus phase should also be marked as the mucus peak.
An increase in temperature observed over at least three consecutive measurements indicates the presence of a two-phase cycle and possible ovulation. After the start of a new menstrual cycle, fertile and infertile days should be determined according to the standard rules.
You should know that the first postpartum menstrual cycles tend to be irregular. They are usually shorter due to a shortened post-ovulatory (luteal) phase, but there are also cycles in which women may have to wait a long time for menstruation to occur.
The use of hormonal contraception after childbirth and during lactation is not recommended. Breastfeeding is a contraindication for combined oral contraceptive pills. However, it is not uncommon for doctors to prescribe breastfeeding women the so-called “mini-pill,” which contains only progestogens. These can reduce both the quantity and quality of the milk produced by the mother. An example is pills containing desogestrel, which, after hydroxylation and reduction to its active metabolite (etonogestrel), is secreted into breast milk in small amounts. It should also be noted that mini-pills do not completely suppress natural menstrual cycles; ovulation still occurs in many women. The effect of progestogen-only pills is mainly limited to changes in the cervix, endometrium, and modifications of fallopian tube function. Therefore, fertilization of the egg can still occur, but the action of the mini-pill prevents implantation of the embryo in the uterine cavity. The effectiveness of this type of contraceptive is also relatively low compared to Multisymptom Fertility Awareness Methods, ranging from 0,3-4,0 (not accounting for anti-implantation effects).