Menopause: when and how a woman's fertility declines
Female fertility, unlike male fertility, is cyclical and periodic in nature. It begins to develop during puberty, then stabilizes, and gradually declines during the premenopausal period.
For women, it is important to know when menopause – the last menstrual period of life – may occur, what the preceding phase (premenopause) looks like, what changes take place in the body at that time, whether conception is still possible, and finally, how one can be certain that menstruation will never occur again.
- In our climate, menopause typically occurs between the ages of 45 and 55, and sometimes even earlier.
- The period preceding menopause (1-2 years) is characterized by irregular menstrual cycles, a deterioration in the quality of cervical mucus secretion, and changes in sensations in the vaginal vestibule.
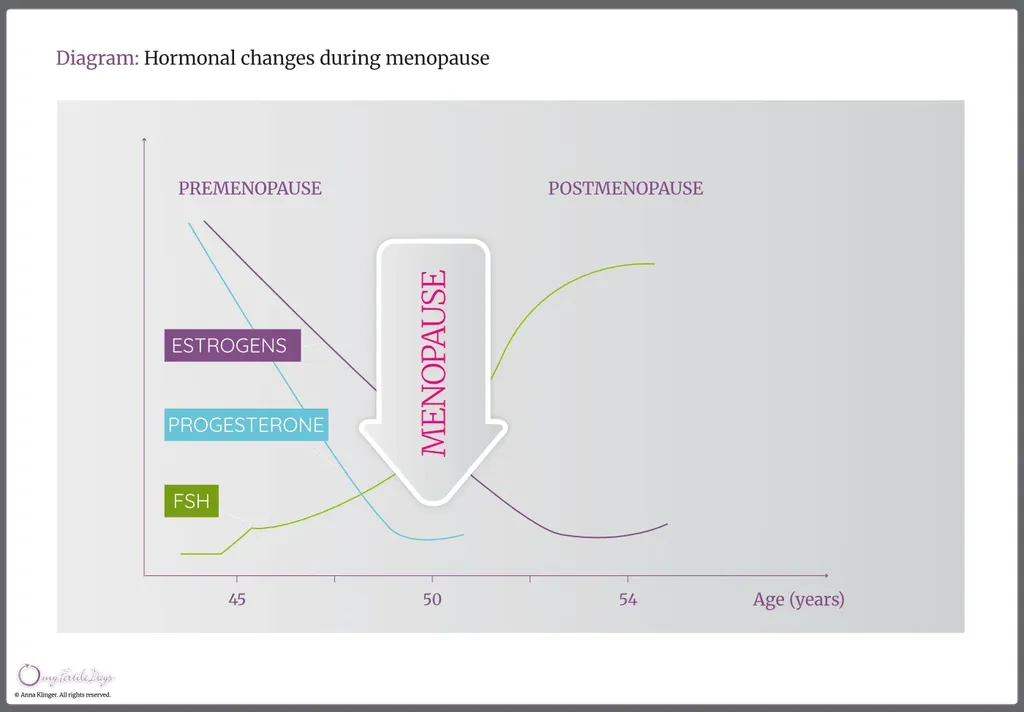
- During premenopause, a woman’s hormonal balance undergoes significant changes – most notably a decline in estrogen levels and a very pronounced drop in progesterone levels.
- These abrupt hormonal changes often lead to troublesome symptoms, known as vasomotor or climacteric symptoms, which are typical of the menopausal transition (climacterium).
- After a woman’s final menstrual period, a marked increase in the level of follicle-stimulating hormone (FSH) is observed.
Factors that may accelerate the onset of menopause include:
- cigarette smoking,
- genetic (hereditary) factors,
- previous surgical removal of the ovaries or uterus,
- serious illnesses and their treatment, such as chemotherapy used in cancer therapy, as well as thyroid disorders, diabetes, and immune system disorders.
The premenopausal period usually lasts 1-2 years, although symptoms characteristic of the climacteric may persist for more than five years. During this time, ovarian function gradually declines, and consequently, a woman’s fertility progressively diminishes.
A characteristic feature of the menopausal transition is a reduced supply of nutrients to the egg cells and a decreased sensitivity of ovarian follicles to stimulation by the hormones FSH (follicle-stimulating hormone) and LH (luteinizing hormone) secreted by the pituitary gland. As ovarian follicles age, they produce progressively lower amounts of estrogens. In response, the hypothalamus increases its activity, further stimulating the pituitary gland, which attempts to maintain estrogen production at previous levels by increasing FSH secretion. As a result, the estrogen phase (the lower-temperature phase) becomes prolonged, and days with cervical mucus secretion may occur repeatedly. Ovulation – and consequently the progesterone phase – appears with significant delay or may no longer occur at all.
Menstrual cycles during the premenopausal period are usually irregular and are often characterized by a shortened progesterone phase (the higher-temperature phase), caused by a more rapid decline in progesterone levels compared with estrogen levels. If no further menstruation occurs within one year after the last menstrual period, menopause can be considered complete and the postmenopausal period has begun. This can be confirmed by measuring FSH levels in the blood. Persistently elevated FSH concentrations, documented in at least three consecutive monthly tests, indicate the cessation of ovarian function and confirm that ovulation will no longer occur. In the following years, even very high levels of FSH and LH are no longer capable of stimulating the growth and maturation of the small number of remaining follicles (the so-called ovarian reserve). As a result, no egg is released from a Graafian follicle, no corpus luteum is formed, and progesterone and estrogen are no longer produced. Consequently, the endometrial lining does not rebuild and therefore does not shed in the form of menstrual bleeding.
Many women approaching menopause wonder whether pregnancy is still possible. During premenopause, the gradual loss of ovulatory function and the decline in estrogen production lead to progressive ovarian failure and thus physiological infertility. Before menopause occurs, menstruation becomes irregular, and only some cycles are ovulatory (biphasic). In addition, progesterone levels essential for maintaining pregnancy are reduced. In summary, conception becomes very difficult but is not impossible. An effective method for identifying fertile days and periods of natural infertility during premenopause is careful observation of one’s own body using a cycle chart.
Read more:
The climacteric period is often characterized by emotional instability, which is closely related to the physiological changes occurring in the body. The troublesome symptoms of this transition are caused by a rapid decline in female hormone levels, mainly progesterone and estrogens.
A decrease in estrogen levels may lead to mood deterioration and can even trigger depression. This is because the concentration of hormones produced by the ovaries influences the level of endorphins, which have analgesic effects and are responsible for a sense of well-being.
Climacteric symptoms may be alleviated through the use of various herbal preparations, supplementation of certain trace elements, minerals, and vitamins, and, in particularly severe cases, individualized hormone therapy under close medical supervision.
Read more: