The phases of the menstrual cycle and associated physiological changes
For many years, the menstrual cycle was thought to be primarily influenced by the moon and to last 28 days – but those days are long gone. Today, a busier lifestyle means that the length of the menstrual cycle can vary considerably. The first phase of the cycle, in particular, is highly sensitive to numerous external factors, such as the type and intensity of light, long-distance travel across time zones with temperature changes, sleep quality, nutritional status, physical fitness, chronic stress, and various health conditions.
The calendar method described by Ogino and Knaus is no longer considered reliable. As a result, it has become increasingly important for each woman to listen to her own body, to be aware of its cyclical changes, and to observe these changes regularly.
The following section of this article will discuss in detail some issues concerning the basic symptoms of fertility:
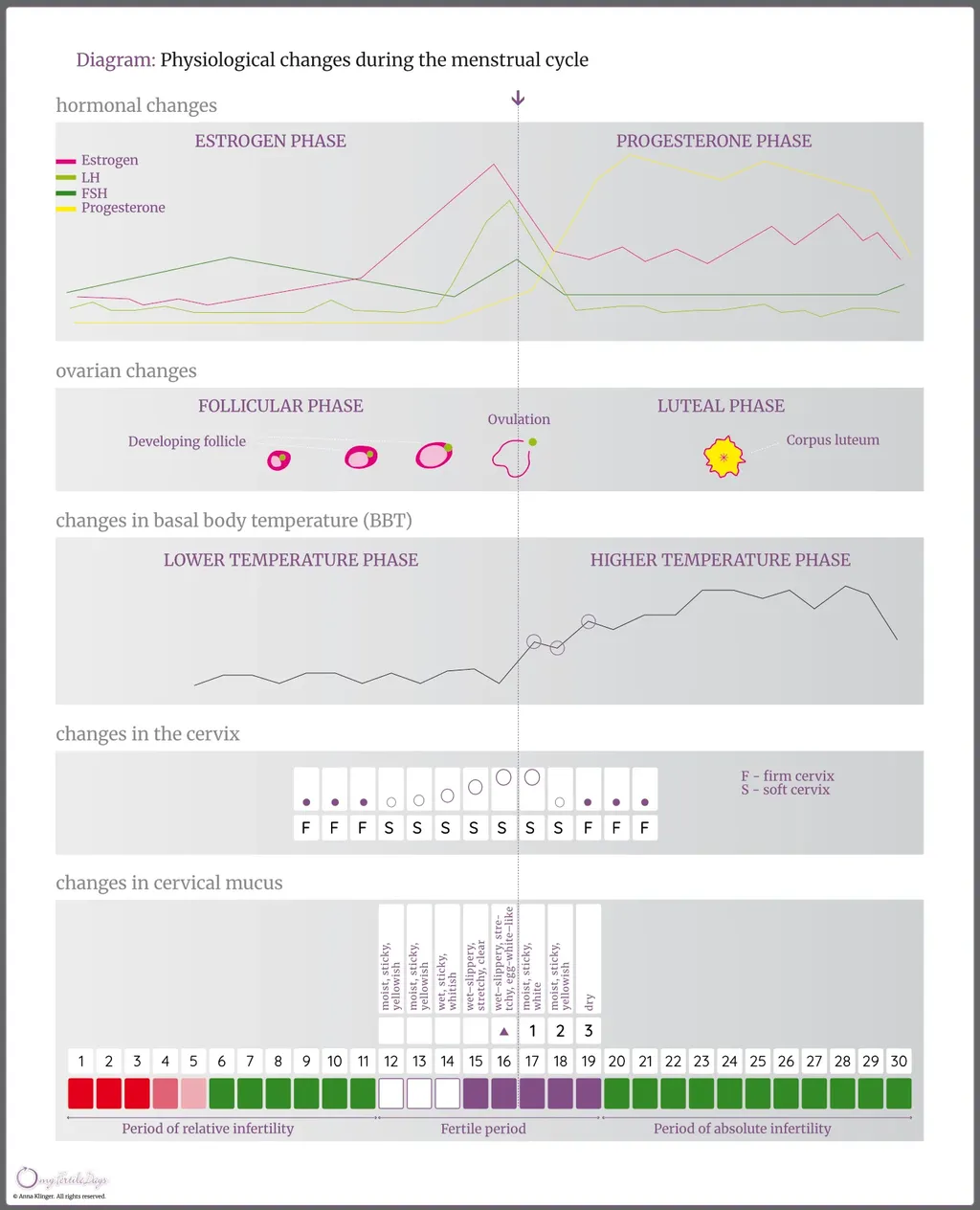
- The typical menstrual cycle is biphasic: it begins with menstruation, followed by the first preovulatory (estrogen) phase, and then the second postovulatory (progesterone) phase.
- Nowadays, cycles lasting between 23 and 35 days are considered typical, whereas cycles are considered irregular when the difference in their length exceeds 10 days. This variability means that determining fertile days based on a standard 28-day menstrual cycle often leads to unplanned pregnancy.
- Hormonal changes cause a number of observable symptoms, including changes in the quality of cervical mucus, changes in basal body temperature, and changes in the cervix. Daily observation of these signs makes it possible to accurately determine infertile phases (both relative and absolute) as well as the fertile phase.
- The ability to fertilize the ovum released during ovulation lasts for up to 12 hours (or up to 24 hours in cases of multiple ovulation). However, due to sperm viability, the fertile period is considered to begin approximately 5-6 days before ovulation.
- During each menstrual cycle, hormones are responsible not only for physiological changes within the female reproductive organs but also for fluctuations in mood, physical and cognitive condition, as well as changes in skin condition and overall appearance. Awareness of these cyclical changes and the ability to recognize them daily can help women better manage periodically occurring discomforts.
The course of a typical menstrual cycle
The menstrual cycle begins on the first day of menstrual bleeding and ends on the day before the next bleeding starts.
A typical menstrual cycle is biphasic, meaning it consists of two successive phases: the preovulatory and postovulatory, separated by ovulation. Contrary to popular belief, ovulation does not usually occur in the middle of the cycle but rather approximately 14 days before the next menstrual bleeding.
During the preovulatory phase (also known as the estrogenic or follicular phase), which begins shortly after menstruation ends, the uterine lining undergoes regeneration as a result of the activity of the dominant hormones of this phase – estrogens. At the same time, ovarian follicles grow and mature; one of them becomes dominant and develops into a Graafian follicle. When it reaches full maturity, the follicle ruptures and releases an egg during ovulation. The released egg is captured by the fimbriae of the fallopian tube and guided inside, beginning its journey toward the uterus. After approximately 12–24 hours, the egg – if not fertilized – degenerates and is expelled.
The postovulatory phase (also known as the progesterone or luteal phase) is dominated by the activity of progesterone. This hormone is produced by the corpus luteum, which develops from the ruptured Graafian follicle, and it is responsible for the secretory transformation of the endometrium. If fertilization and implantation of the fertilized ovum do not occur, the corpus luteum regresses, progesterone levels fall, and ischemia of the endometrial lining ensues. This leads to its shedding, which manifests as menstrual bleeding and marks the beginning of the next menstrual cycle.
Menstruation prepares the uterus for the subsequent cycle, during which the endometrial lining rebuilds and transforms again to create conditions suitable for possible embryo implantation.
Currently, menstrual cycle length often differs from the average 28-day cycle, and cycles lasting between 23 and 35 days are considered typical. Cycles are regarded as irregular when the difference in their length exceeds 10 days. Variations in cycle length occur primarily in the preovulatory phase, whereas the postovulatory phase is relatively stable and typically lasts about 14 days.
Consequently, identifying fertile days based solely on the date of the last menstrual period and calculations using a standard 28-day cycle may be inaccurate and often result in unplanned conception. Only comprehensive observation of the signs and signals of the female body allows for accurate determination of fertile days. Therefore, learning to recognize these signals and the physiological processes that regulate them is highly recommended.
Hormonal changes associated with the particular phases of the menstrual cycle
The transformations that occur during the menstrual cycle are driven by hormonal changes. Hormones are chemical messengers secreted by endocrine glands in response to signals initiated by the brain, and they influence various functions throughout the human body.
Each menstrual cycle consists of two phases: the preovulatory phase, dominated by estrogen activity, and the postovulatory phase, in which progesterone plays the major role.
At the beginning of each cycle, following the onset of menstrual bleeding, the hypothalamus stimulates the pituitary gland to produce follicle-stimulating hormone (FSH). This hormone initiates the maturation of ovarian follicles. As the follicles mature, they also secrete estrogens, which promote regeneration and growth of the endometrium, increase cervical mucus secretion, and cause the cervix to rise, soften, and slightly open. High estrogen levels do not affect basal body temperature, which remains relatively low during this phase.
The concentration of estrogens reaches its peak approximately 24 hours before ovulation. At the same time, there is a sudden surge of luteinizing hormone (LH) released by the pituitary gland. This LH surge causes the rupture of the mature (Graafian) follicle and the release of the egg (ovulation). If the LH surge does not occur or is insufficient, ovulation will not take place, even if the follicle has matured.
After ovulation, estrogen levels fall rapidly, reaching a minimum, then rise slightly again and remain below preovulatory levels until menstruation. The follicle that released the egg transforms into the corpus luteum, which secretes progesterone. Elevated progesterone levels are associated with further thickening of the endometrium and increased blood supply, inhibition of further ovulation, a rise in basal body temperature of at least 0.2°C, thickening of cervical mucus, and lowering, closing, and firming of the cervix. These changes constitute the set of signs used to identify the beginning of the postovulatory infertile phase (absolute infertility).
The corpus luteum secretes progesterone for approximately two weeks. If fertilization does not occur, it regresses, progesterone levels drop rapidly, and ischemia of the endometrium follows. This leads to shedding of the uterine lining, which manifests as menstrual bleeding. If fertilization occurs, the corpus luteum of pregnancy develops and continues to secrete progesterone for about 16 weeks, until the placenta is fully functional, after which it gradually regresses.
How do you ovulate and how can you determine the moment of ovulation?
Within the ovaries, follicles exist at various stages of development. The majority are primary follicles, which each female is endowed with during fetal life. Their number gradually decreases over time until they are depleted during the premenopausal period.
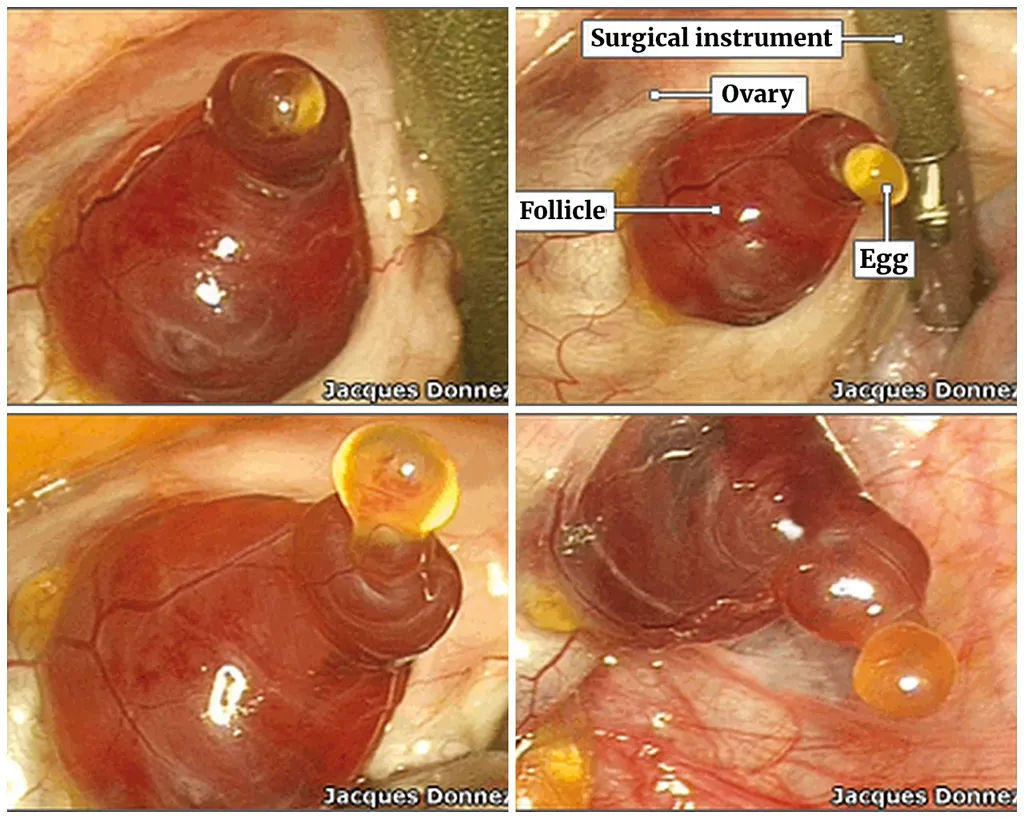
Under the influence of FSH, primary follicles develop into growing follicles; several progress toward maturity, and typically one becomes the dominant Graafian follicle, which releases the egg during ovulation.
During the periovulatory period, cervical mucus exhibits its most fertile characteristics: it becomes highly stretchy, clear, slippery, and gives a sensation of wetness, resembling raw egg white. After the Peak Day – the last day of the most fertile mucus – the quality of mucus declines rapidly and soon disappears.
Ovulation is a complex process involving numerous hormonally active substances and may be disrupted under various conditions. The exact moment of ovulation is difficult to determine precisely. Indicators suggesting imminent ovulation include follicular growth observed by ultrasound, rising LH levels, and changes in cervical mucus characteristics. Ovulation is assumed to have occurred based on increased progesterone levels and a sustained rise in basal body temperature; however, in some cases (such as luteinized unruptured follicle syndrome, LUF), these signs may be present without actual ovulation.
Using natural fertility awareness methods developed by Prof. Josef Rötzer, the timing of ovulation can be estimated quite accurately. This approach is based on daily observation of cervical mucus and basal body temperature measured immediately after waking. Ovulation is assumed to occur on the Peak Day, the day following it, or on the day of the temperature dip preceding the sustained temperature rise, or on the first day of elevated temperature.
However, the only definitive confirmation of ovulation is direct observation during surgery or the occurrence of pregnancy.
The egg released during ovulation remains viable for approximately 12 hours (up to 24 hours in cases of multiple ovulation). Further ovulation within the same cycle is inhibited by progesterone secreted by the corpus luteum formed after the rupture of the Graafian follicle.
The moment of ovulation (it lasted 15 minutes) was recorded incidentally during a hysterectomy (source: Ovulation moment caught on camera).
During another surgery, the moment of ovulation has been successfully recorded:First ever footage of human ovulation
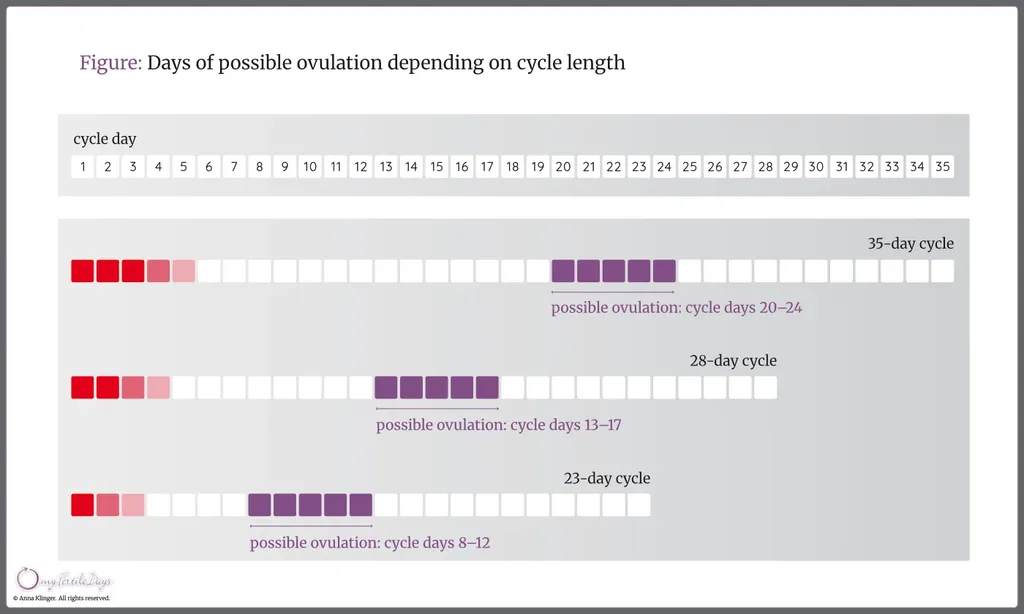
The figure below presents the possible ovulation days, depending on the length of the cycle – usually they are between the 12th and 16th day before the next period.
How do the hormones dominant during the different cycle phases affect the cervix and its mucus?

The structure and function of mucus secreted in the cervical crypts (glands located along the cervical canal) and its relationship to fertility were examined and described by Prof. Erik Odeblad of the University of Umeå in Sweden. He identified four distinct types of cervical mucus: G, L, S, and P.
The G-type mucus is thick and dense. It closes the cervical canal during infertile days and acts as a barrier to sperm. It typically occurs immediately after menstruation, during the postovulatory phase, and during pregnancy. P-type mucus, produced in the highest cervical crypts, dilutes G-type mucus. This dilution causes a sensation of moisture in the vaginal vestibule (referred to as the “W” sensation in Rötzer’s method) and marks the beginning of the fertile phase. As estrogen levels rise, L-type mucus appears. It is sticky, stringy, and opaque. With further increases in estrogen concentration, the mucus becomes progressively clearer, more elastic, and produces a sensation of lubrication and slipperiness – this is S-type mucus. At the same time, estrogen causes the cervix to soften and open slightly, facilitating sperm passage into the uterus and onward to the fallopian tubes.
Periovulatory mucus contains both strands of S-type mucus (a liquid gel) and clusters of L-type mucus (a sticky gel). The balance between these two types appears to be essential for optimal fertility. According to Prof. Odeblad, particles of L-type mucus form a structural framework for the smooth S-type mucus and function as a selective filter, trapping less viable sperm while facilitating the transport of more efficient sperm. Near ovulation, cervical mucus secretion consists primarily of S and L types, with approximately 4–8% P-type mucus, which intensifies the sensation of slipperiness by diluting the other mucus types. This combination facilitates sperm transport into the uterine cavity. The presence of P-type mucus explains why a strong sensation of lubrication may occur even when little or no visible mucus is observed externally – a situation often corresponding to the Peak Day.
After ovulation, progesterone secretion causes the cervix to firm and close rapidly, creating a so-called biological valve that prevents sperm entry. An additional barrier is formed by the thick, sticky G-type mucus.
Prof. Odeblad’s observations also indicate that the length of the fertile mucus phase changes with age. In women around 20 years old, this phase lasts an average of 4–5 days, whereas in women aged approximately 35 years, it typically lasts only 1–2 days. The qualitative characteristics of cervical mucus also change accordingly.
Based upon:
- E. Odeblad „The Discovery of different types of cervical mucus and the Billings Ovulation Method”, Bulletin Natural Family Planning Council of Victoria, 1994.
- E. Odeblad “Cervical Mucus and their functions”, Irish College Physicians and Surgeons, 1997.
See more:
What is the basal body temperature chart?
By observing a basal body temperature (BBT) chart throughout the menstrual cycle, two distinct phases can be identified: a lower-temperature phase and a higher-temperature phase.
The lower-temperature phase begins in the early days of menstruation. Shortly after ovulation, basal body temperature rises and remains elevated until the onset of the next menstrual period.
This postovulatory rise in basal body temperature is caused by progesterone, which is produced by the corpus luteum formed after the rupture of the Graafian follicle. Progesterone prepares the body for implantation of a fertilized egg and supports the proper development of pregnancy. In a non-fertile cycle, the menstrual corpus luteum remains active for about 10 days before it begins to regress, leading to the shedding of the upper layer of the endometrium and its expulsion as menstrual bleeding.
If fertilization occurs, the corpus luteum becomes the corpus luteum of pregnancy. It produces large amounts of progesterone and estrogens, which are essential for maintaining pregnancy. Elevated progesterone production continues until approximately the 16th week of pregnancy, when the fully developed placenta takes over the role of pregnancy maintenance.
The primary function of progesterone is to reduce uterine contractility and prevent premature expulsion of the fetus. Toward the end of pregnancy, a decline in progesterone activity signals the onset of labor.
See more:
When are your fertile and infertile days?
During the menstrual cycle, three phases associated with changes in fertility can be distinguished:
The relative infertility phase. This phase begins with menstruation. Its end can be determined using several basic principles based on observation of basal body temperature measured after waking and the quality of cervical mucus. The length of this phase is not constant and may vary from cycle to cycle. In very short menstrual cycles, follicular development may begin very early, and the fertile phase can start in the final days of menstruation. The Pearl Index for this phase is less than 0.2%.
The fertility phase, lasts relatively short. During this time, a mature egg is released from a Graafian follicle (ovulation) and travels through the fallopian tube. The egg remains capable of being fertilized for up to 12 hours (or up to 24 hours in cases of multiple ovulation). Because sperm can survive for 5-6 days, the fertile period is considered to begin several days before ovulation. Easily observable signs of fertility include high-quality cervical mucus, changes in the cervix, and ovulatory pain.
The postovulatory (absolute) infertility phase begins a few days after ovulation, following the degeneration of the egg, and lasts until the next menstruation. The end of the fertile period is marked by a sustained rise in basal body temperature of at least 0.2°C observed over three consecutive measurements, along with a marked decline in the quality of cervical mucus and its rapid disappearance. The Pearl Index for this phase is 0%, indicating absolute infertility.
The influence of hormones on your mood and appearance
During the menstrual cycle, natural hormonal fluctuations in a woman’s body activate reproductive processes that are reflected in changes within the reproductive organs, external appearance, and physical, emotional, and cognitive functioning.
The activity of estrogens during the first (preovulatory) phase of the cycle results in:
- maintenance of basal body temperature at an unchanged low level,
- gradual regeneration of the endometrium,
- lifting, softening, and opening of the cervix,
- progressive changes in cervical mucus from less fertile to more fertile.
During the period of highest estrogen levels, many women experience improved mood, increased physical energy, greater efficiency, enhanced concentration, increased libido, and a generally more attractive appearance. However, the estrogen phase is relatively unstable, varies from cycle to cycle, and is particularly sensitive to stress, medication, and other external factors that may disrupt it.
In contrast, the increased concentration of progesterone in the second (postovulatory) phase of the cycle leads to:
- an increase in basal body temperature of at least 0.2°C,
- inhibition of further ovulation,
- a sensation of breast fullness,
- secretory changes in the endometrium in preparation for possible embryo implantation,
- closing, lowering, and firming of the cervix,
- thickening of cervical mucus.
During the progesterone phase, women may more often experience decreased physical and emotional well-being, fatigue and sleepiness, increased irritability, reduced concentration and cognitive performance, decreased libido, and skin problems.