How to conduct self-observation and how to interpret the fertility changes in your menstrual cycle?

During the menstrual cycle, a woman’s body produces hormones whose concentrations vary depending on the phase of the cycle. These hormonal changes influence the functioning of the female reproductive organs and, consequently, fertility. Daily observation of the physiological changes that occur cyclically in the body provides the information needed to accurately determine fertile days and periods of natural infertility. Regular self-observation and recording of these changes help to better understand how the body works, support acceptance of these natural processes, and allow early identification of any abnormalities or cycle disorders.
In the following section, you will learn how to observe fertility indicators throughout the menstrual cycle and how to interpret their changes correctly:
- Basal body temperature should be measured every day at the same time, using the same thermometer and the same method. It is usually taken in the morning, immediately after waking. However, it is also possible to obtain a reliable temperature chart if you work shifts, provided that the measurement is preceded by at least one hour of uninterrupted rest.
- Observation of cervical mucus should be carried out throughout the entire day, ideally during each visit to the toilet. On the cycle chart, the most fertile type of mucus observed during the day is recorded, along with the accompanying sensation.
- Cervical self-examination is an additional, complementary observation. It is usually performed once during the day and once in the evening. Although it may initially cause some hesitation, it can be especially helpful for premenopausal women or for those who have difficulty noticing mucus on the external genital area.
- During the preovulatory phase, estrogens are the dominant hormones. They cause the cervix to soften and open slightly and stimulate the production of cervical mucus, whose function is to facilitate sperm transport into the uterine cavity and onward to the fallopian tubes. Estrogens do not affect basal body temperature, which therefore remains at a consistently low level.
- During the postovulatory phase, progesterone becomes the dominant hormone. It causes the cervix to close and firm and leads to the disappearance of fertile mucus, creating a barrier to sperm. Rising progesterone levels after ovulation also cause basal body temperature to increase by at least 0.2°C. This higher temperature level is maintained for approximately 14 days, until the next menstrual period. Progesterone additionally prevents further ovulation within the same cycle.
Basal body temperature measurement
Years of research into the physiology of the female menstrual cycle have shown that changes in the concentrations of hormones produced during each cycle are closely linked to changes in basal body temperature. During the first, estrogen-dominated phase, body temperature remains relatively low and stable. In the second, progesterone-dominated phase, it rises by at least 0.2°C. Observing basal body temperature (BBT) therefore provides valuable information about the current phase of the menstrual cycle.
Basal body temperature should be measured immediately after waking and before engaging in any physical activity. Ideally, it should be taken after at least six hours of uninterrupted rest. While this is not an absolute requirement, very short sleep may cause irregular or less reliable readings. It is also important to remember that body temperature naturally begins to rise around 7:30 a.m., so measurements taken after this time may be higher. Shift workers can also obtain reliable temperature charts. If you sleep during the day after night work, measure your temperature immediately after waking and record the time of measurement. Alternatively, you may choose a fixed measurement time; however, you should rest lying down for at least one hour before taking the measurement and always note the measurement time. The measurement time should not vary by more than one and a half hours.
Temperature should be measured inside the body: orally (in the mouth), vaginally, or rectally. Measurements taken under the arm, in the ear, or on the forehead are unreliable and should be avoided. If measuring orally, it is essential to place the thermometer in exactly the same spot each day.
Any type of thermometer may be used, but it is important to be aware of the specific characteristics of each type:
- electronic thermometers measure temperature quickly but may have an uncertainty of up to 0.1°C.;
- ovulation thermometers (digital or analog) provide an accurate reading after approximately 3 minutes;
- mercury ovulation thermometers require about 4 minutes for oral measurement and 2 minutes for vaginal or rectal measurement;
- standard medical mercury thermometers should be used for about 8 minutes orally or 5 minutes vaginally or rectally.
Do not discontinue temperature measurements during illness. If a sudden temperature rise is caused by illness, other observed symptoms and cycle signs will usually allow for an accurate interpretation of the menstrual cycle phases.
Temperature chart interpretation
Menstruation is preceded by a period of at least three elevated temperatures, although for most women the high-temperature (corpus luteum) phase lasts approximately 14 days. With the onset of menstruation, basal body temperature usually drops and remains at a low level until ovulation. The baseline is determined by the highest of the six temperatures preceding the temperature rise. A temperature rise indicates that ovulation has already occurred – that the Graafian follicle has ruptured and the corpus luteum has begun producing progesterone. The higher-temperature level is defined as at least 0.2°C above the baseline. To confirm the postovulatory phase, the elevated temperature must be sustained for at least three consecutive days after the mucus Peak Day. It is assumed that immediately after these days, the phase of absolute infertility begins.
In some cycles, temperature may begin to rise while fertile-type cervical mucus is still being observed. This situation is known as an early temperature rise. Such temperatures should be marked with a ↑ symbol on the cycle chart. They result from the body’s sensitivity to progesterone secreted by the granulosa cells of the Graafian follicle. These cases highlight the importance of considering the mucus Peak Day in interpretation. In the method developed by Prof. J. Rötzer, "elevated" temperatures are only confirmed after the Peak Day and are then circled on the chart as certain observations. If the third elevated temperature does not reach at least 0.2°C above the baseline, the determination of the infertile phase should be postponed until the fourth elevated temperature, provided that it remains above the baseline. If, after the Peak Day, one of the three elevated temperatures falls to the baseline or below, that measurement should be disregarded and the next elevated temperature should be awaited. Temperature rises caused by illness, stress, travel, or time-zone changes – whether lasting one or several days – should be marked as disturbed (placed in brackets) and must not be used when determining the baseline. A single disturbed temperature may still be included when counting the six lower temperatures preceding the temperature rise.
Cervical mucus observations
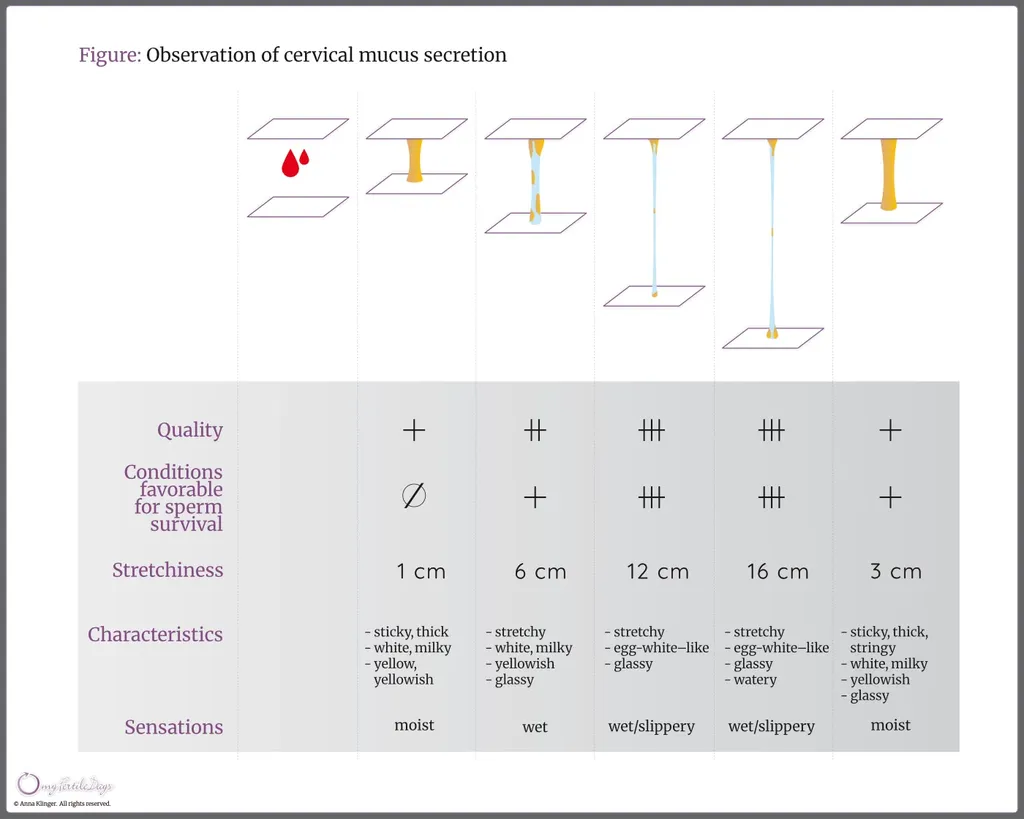
Under the influence of sex hormones, cells of the cervix produce cervical mucus, which may also be visible on the external genital area. Cervical mucus can vary in texture, color, and the sensations it produces in the vaginal vestibule. These characteristics depend on which hormone is dominant at a given phase of the menstrual cycle. External observation of cervical mucus is simple: during each visit to the toilet, observe the secretion visible on the toilet paper.
Evaluate the mucus by noting its color, texture, and the sensation felt in the vaginal vestibule. If several mucus characteristics are observed during the same day, record the one that is most fertile, meaning the type that provides the most favorable conditions for sperm survival and movement.
Cervical mucus secretions of a less fertile type have the following characteristics:
- opaque, non-transparent appearance, whitish, milky, or yellowish color;
- sticky, thick, or lumpy texture;
- sensations of dryness or slight moisture.
Cervical mucus secretions of a more fertile type have the following characteristics:
- transparent, glassy, or crystal-clear appearance;
- egg-white–like consistency;
- stretchiness (from about 2 cm up to 15 cm), smooth and elastic texture;
- sensations of moisture, wetness, or wet-slippery.
Sensations felt in the vaginal vestibule often provide more valuable information than the visible mucus itself. For example, the “W” sensation (“watchful awareness”), considered the first sign of fertility in Rötzer’s method, and the “wet-slippery” sensation, which may occur even when little or no mucus is visible externally. In such cases, mucus is extremely smooth and produces an intense feeling of lubrication. All observations of cervical mucus and accompanying sensations should be recorded on the cycle chart using the appropriate symbols.
Interpretation of cervical mucus characteristics
The appearance of any cervical mucus is always a sign of the beginning of the fertile period, whereas dry days are considered days of natural infertility. As estrogen levels increase, the type of mucus changes from less fertile to more fertile, until it reaches its optimal characteristics – namely, being transparent, stretchy, wet, and slippery.The last day on which any of the most fertile mucus characteristics are observed is defined as the mucus Peak Day and is marked with ●. This day serves as the reference point for determining the beginning of the postovulatory infertile phase: the third evening of sustained higher temperatures after the Peak Day marks the end of the fertile period.
It is important to remember that the menstrual cycle is dynamic and can be influenced by various factors such as stress, illness, medication, excessive alcohol consumption, lack of sleep, or changes in climate and time zones. Such disturbances may be reflected in mucus observations. They most often occur during the first phase of the cycle, when the dominant ovarian follicle is growing and maturing. In some cases, despite hormonal changes and the presence of fertile-type mucus, ovulation does not occur. After several days, the follicular maturation process may begin again, fertile mucus reappears, ovulation finally takes place, and a temperature rise follows. This phenomenon is known as delayed ovulation.
Some women may experience light bleeding lasting a few days while observing fertile-type mucus. This bleeding should not be considered menstrual bleeding. This is referred to as mid‑cycle bleeding and is defined as bleeding that is not preceded by a high‑temperature phase and occurs during the low‑temperature phase. It is important to note that mid-cycle bleeding coincides with possible fertility, and the bleeding may obscure the presence of cervical mucus. If, after such bleeding, no mucus is observed, the last day of bleeding is considered the Peak Day and should be marked with ●.
Self-examination of the cervix
Some women have difficulty observing cervical mucus on the external genital area. In such cases, cervical self-examination is recommended as an additional and complementary element of fertility sign observation, particularly within the Rötzer method. By examining the cervix through touch, you can monitor the changes that occur during the different phases of the menstrual cycle. Although this examination may initially cause hesitation or discomfort, it provides valuable information about natural periods of fertility and infertility.
Observations are best performed in the evening. Before beginning, make sure your hands are thoroughly washed and your fingernails are short. The most suitable time to start cervical self-examination is during the postovulatory phase, when the cervix is lower and more easily accessible. The uterus can be imagined as an inverted pear, with the external opening of the cervix resembling the narrower end of the pear, featuring a small indentation in the center. During the infertile phase, the cervix is firm – often compared to the tip of the nose – whereas during the fertile phase it becomes soft, similar in consistency to an earlobe. While examining the cervix, you may also observe cervical mucus collected at its opening. During the fertile period, changes in the cervix – such as softening and slight opening – facilitate sperm entry into the uterus. In contrast, during infertile phases, thick, infertile-type cervical mucus forms an effective barrier to sperm. It is important to note that cervical self-examination may interfere with external mucus observations. Therefore, you should choose either to observe mucus externally or to perform cervical examination with assessment of mucus collected from the cervical opening, but not both at the same time.
Interpretation of changes in the cervix
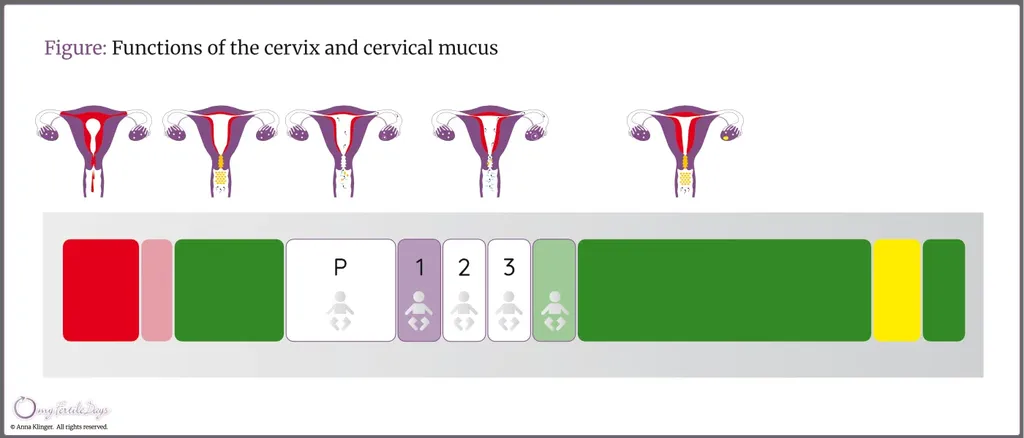
At the beginning of menstruation, the cervix, under the pressure of the menstrual flow, releases a thick mucus plug. During the natural infertile periods (marked in green in the figure below), the cervix is firm, closed, and positioned low in the vagina. Thick and sticky G-type mucus, which accumulates again, forms an additional barrier that prevents sperm from entering the uterine cavity.
As estrogen levels increase, noticeable changes occur in the cervix: it begins to open, becomes softer, rises higher, and may become more difficult to reach during self-examination. Under the influence of smooth P-type mucus, the thick and sticky G-type mucus becomes diluted, and more fertile L-type mucus appears. This marks the beginning of the fertile days (shown in the figure as areas outlined in purple).
As ovulation approaches, mucus that supports sperm survival and creates channels for their transport (S-type mucus) can be observed. At the same time, abundant, slippery P-type mucus is secreted, facilitating the movement of sperm into the uterus and fallopian tubes. This mucus is often so fluid and smooth that it may be barely visible, producing mainly an intense sensation of moisture and lubrication.
After ovulation, the cervix closes rapidly, becomes firm again, and moves downward. Thick mucus accumulates at the cervical opening, often causing a sensation of dryness during examination. Typically, three days after the mucus Peak Day, the phase of natural infertility begins (marked in green in the figure). Shortly before the next menstrual period, a sensation of moisture may again be felt in the vaginal vestibule, and cervical mucus secretion – often yellowish in color – may appear. This is caused by falling progesterone levels and a temporary dominance of estrogens.
See more: