Self-observations of fertility symptoms during the premenopause period

Premenopause (the period preceding menopause, which is marked by the last menstrual period in a woman’s life) is a natural stage in every woman’s life. It is characterized by a gradual decline in ovarian activity and a progressive reduction in fertility.
- During premenopause, menstrual cycles may become shortened, often with a shortened progesterone (luteal) phase, or prolonged, sometimes lasting 40, 60, or even 90 days. These longer cycles are usually the result of an extended estrogen (follicular) phase caused by disturbances in follicular development.
- Anovulatory, single-phase cycles are also common during this period. Basal body temperature charts may appear irregular, with fluctuating or “bouncing” temperature patterns.
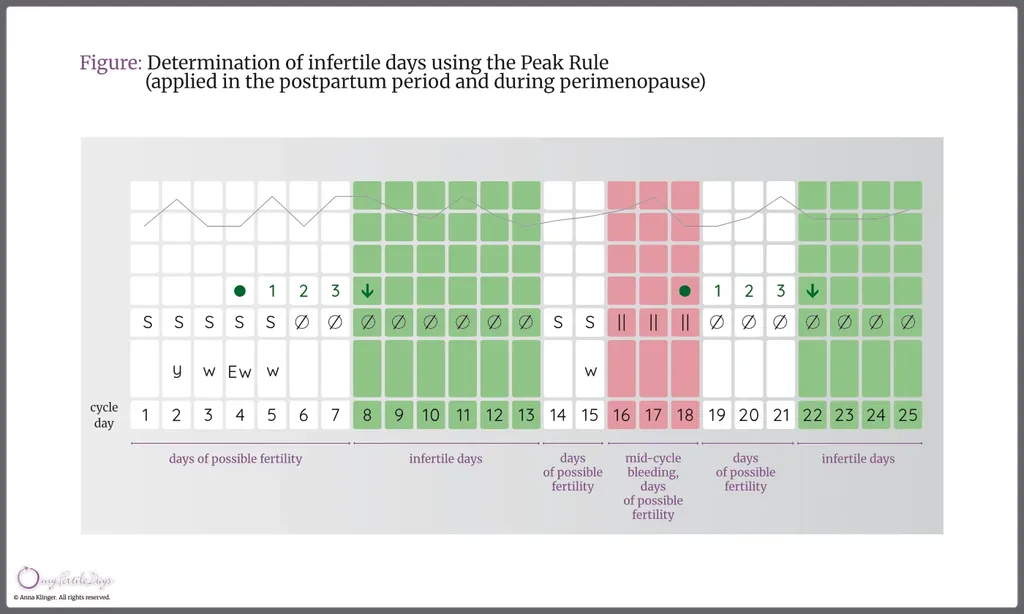
- To determine infertile periods during premenopause, the mucus peak rule is used: the infertile phase begins on the evening of the fourth day after the cervical mucus peak. Calculation-based rules are not applied during this stage of life.
- During the menopausal transition, cervical mucus may become scant, difficult to observe, and less fertile in quality, making the identification of a clear mucus peak more challenging. In some cases, however, the mucus appearance may remain relatively unchanged.
- Changes also occur in the cervix itself: it typically remains closed, firm, dry, and positioned lower in the vaginal canal.
During premenopause, menstrual cycles become increasingly irregular as ovarian activity gradually declines and the production of reproductive hormones – estrogens and progesterone – decreases.
In the early stage, the phase of higher temperatures (the progesterone or luteal phase) may become shortened. This occurs because progesterone levels decline more rapidly than levels of estrogen. As a result, the overall length of the menstrual cycle may shorten.
Later, a lengthening of the lower‑temperature (estrogen or follicular) phase can be observed. This is caused by a reduced sensitivity of the ovarian follicles to follicle‑stimulating hormone (FSH). Poor follicular growth is associated with lower estrogen levels in the blood, which triggers increased stimulation from the pituitary gland through elevated FSH secretion. This surge in FSH may stimulate the growth of several follicles, leading to a temporary rise in estrogen levels. Consequently, cycles may include multiple days of fertile‑type mucus or episodes of intermenstrual bleeding, while the follicular (lower‑temperature) phase becomes prolonged, resulting in longer cycles. However, full follicular maturation and ovulation occur less frequently during this stage.
During premenopause, herbal preparations containing chasteberry (Vitex agnus‑castus) are sometimes considered. They are commonly used to support the regulation of irregular menstrual cycles, ease premenopausal symptoms, and help maintain hormonal balance.
After the age of 40, when cycles often become irregular or single-phase, careful and consistent self-observation is especially important. To determine the phase of absolute infertility during premenopause, the same rule used during breastfeeding can be applied – the mucus peak rule. This involves identifying the cervical mucus peak and then waiting four full days. The evening of the fourth day marks the beginning of the infertile phase, provided that no new fertility signs or temperature rise are observed. If cervical mucus reappears, those days must be treated as potentially fertile, and the peak must be identified again. The four-day waiting period should then be repeated to determine the onset of infertility.
As a result of pituitary hyperstimulation by FSH, estrogen levels may rise high enough for the cervical cells to produce fertile‑type mucus or for intermenstrual bleeding to occur. However, in the period preceding menopause, the characteristics of cervical mucus gradually deteriorate. Less fertile‑type mucus is most commonly observed, and in some women the sensation of moisture appears only briefly. In such cases, both of these signs should be treated as the peak day. The hormonal changes occurring during premenopause affect not only the nature of cervical mucus but also the cervix itself, which typically becomes closed, dry, and lower in position.
It should be noted that ovulation may still occasionally occur, and a temperature rise may appear on the chart. To determine the post‑ovulatory infertile phase, the standard rules of the Rötzer method are applied: we wait for three higher temperatures occurring after the peak day of cervical mucus symptoms, with no accompanying signs of fertility. Some women continue to have normal biphasic cycles even after the age of 50; however, conceiving a child at this age is significantly more difficult due to reduced levels of estrogen and progesterone, which are necessary for the proper development of pregnancy.
Prepare for the possibility of a very long phase of lower temperatures, after which the higher‑temperature phase may appear with a significant delay – or may no longer appear at all. When the intervals between bleeding become longer, fertility signs will occur less and less frequently, and higher‑temperature phases will almost completely disappear. At this point, it is advisable to check the FSH level in the blood. As ovarian function declines, the level of FSH – follicle‑stimulating hormone, which promotes the maturation of the ovarian follicle – rises sharply. Persistently high values of this hormone, confirmed several times at monthly intervals, indicate that ovulation will no longer occur.