

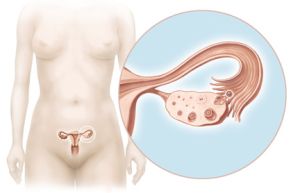
Ovulation is a process of releasing a ready for fertilization egg (ovum) from a mature ovarian follicle, called the Graafian follicle. This is the culmination of each menstrual cycle, without which it is impossible to conceive a new life.
Read about ovulation process, its symptoms and ovulation disorders.
Preparation for ovulation
Before ovulation the whole process of growth and follicular maturation must take place in your ovaries. From hundreds of thousands of primary (primordial) immature follicles continuously present in woman’s ovaries from her birth (and even before her birth in a fetus stage) a group of rising follicles begins to develop. Soon one of them begins to dominate and be ahead of the others in the development stage. When the dominant follicle reaches a diameter of about 10 mm, it is growing on average 2 mm per day (for 6-7 days). When it has at least 20-26 mm is called a mature Graafian follicle and is ready to rupture.
The process of maturation of ovarian follicles is stimulated by a follicle-stimulating hormone FSH (follitropin), secreted by the pituitary gland into the blood.
How do you ovulate
Rising and developing ovarian follicles produce estrogen hormones, which blood levels gradually increase, reaching a maximum level about 36 hours before the ovulation. After that the pituitary gland ejects certain quantities of luteinizing hormone LH (lutropin), which are essential for the ovulation to take place. This ejection precedes ovulation for about 24-36 hours, while its peak for about 12-24 hours.
The ovulation tests that are available in pharmacies operate similarly - helping you to detect the LH peak. The most appropriate time to conceive a baby is 2nd and 3rd day following detection of the LH peak.
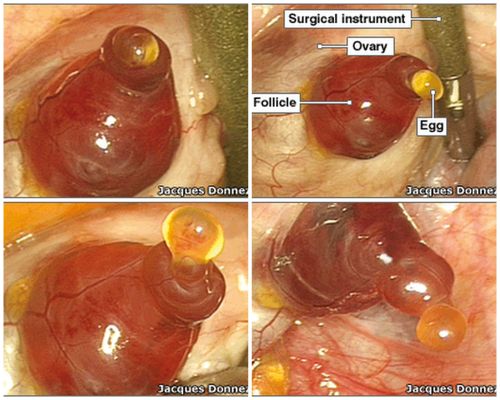
This is the moment of ovulation registered during hysterectomy surgery:
After ovulation, LH stimulates the cells of the corpus luteum, formed from the ruptured Graafian follicle, to produce progesterone which blocks the next occurrence of ovulation in this menstrual cycle.
The phase from ovulation to next period, called the luteal phase, may have a length from 11 to 16 days (for one woman it is fixed). Its shortening may indicate the infertile cycle, while its extension may indicate that you are pregnant.
Ovulation symptoms
Increasing levels of LH in the blood stimulates follicle cells to produce estrogen hormones, which high blood levels causes a few changes in your body, easily to observe:
• softening, opening and lifting of the cervix,
• changes in mucus produced in the crypts of the cervix, that provides the survival of sperm, and thus its liquidation, thinning, clarity and ability to stretch, giving the feeling of wetness and slipperiness (the last day of that kind of cervix mucus observed is called the Peak Day),
• ovulation usually take place in the Peak Day (38%), but can also occur on the 3 days before and 3 days after the Peak Day[1],
• usually just after ovulation occurs the body temperature increase into a direction of the higher temperatures level,
• in peri-ovulatory phase you can feel a semi-ovulatory pain and can observe increased libido, but they are only secondary symptoms, not pointing directly at the moment of ovulation.
Optimal time of fertility (the fertile window) includes a 6-day phase with the presence of cervical mucus and ended with the ovulation day. The best chances of conceiving a baby are if you have intercourse for 2 days before ovulation[2], but the exact moment of ovulation (it usually takes about 15 minutes) is difficult to precisely determine at home. The only sure proof that ovulation really took place is to observe the released egg during a surgery, during the ultrasound monitoring of a menstrual cycle, and… a presence of pregnancy;)
When the ovulation occurs in your menstrual cycle?
If you systematically observe the biomarkers in your menstrual cycle you will not have any problems to determine the time of ovulation:
• the closest to the day of ovulation is the Peak Day and the next day, and also the first day of high temperatures and the day before the temperature begins to increase,
• some kind of confirmation that ovulation occurred is the increase of your basic body temperature to the level of higher temperatures, sustained for at least three days (two-phase fertile cycle).
Disorders of ovulation
To the ovulation occurrence there is necessary a strong increase of the luteinizing hormone level (LH), without its surge Graafian follicle cannot break, even when it reaches a fairly substantial size. Also, if the process of follicular maturation is disturbed at the stage of dominant follicle (eg, by stress or illness), it can lead to delay ovulation, or even the disappearance of a dominant follicle. Preparing for the process of ovulation is very sensitive to interference and therefore the egg may not be released from the mature follicle despite the LH peak. There are also several ovulation disorders[3]:
• The unruptured luteinized follicle (LUF) - the Graafian follicle, which does not release an egg, and turnes into a normally functioning corpus luteum (Ober 1957, Marik and Hulka, 1978),
• The ovum retention - retention of the egg; in this case the Graafian follicle ruptures, but the egg is retained in the surface of the follicle and trapped in the emerging corpus luteum (Craft 1980, Stanger and Yovich, 1984),
• An empty follicle - the mature ovarian follicle ruptures, but there is no egg inside (Rauscher and Ulm, 1963, 1989 and Hilgers 1992, Tulloch 1986, Tsuiki, 1988).
How the ovulation is blocked during hormonal contraception?
Hormonal contraception was originally invented to prevent ovulation and thus prevent pregnancy. Large amounts of synthetic hormones (equivalent of estrogen and progesterone) are inhibit the secretion of natural hormones LH and FSH by the pituitary gland and thus create a kind of “hormone prosthesis” instead of the natural cycle of hormonal changes.
The first birth control pill in 1960 contained a large concentration of synthetic hormones and actually blocked ovulation, but also caused serious side effects and even life threatening. Up today producers tend to gradually reduce the levels of artificial hormones in contraceptive formulations, but the dangerous effects are still significant.
What even more important, many studies have shown that hormonal contraceptives do not always block the occurrence of ovulation. With combined-component pills ovulation may occur in 2-5% of cases, but one-component pills (so-called low dose or mini pills) block ovulation much less effectively – ovulation may occur even in 10-40% of cases[4]. The present study found that in such cases other mechanisms of contraceptives should act, mainly operating on the uterus lining, making it unfriendly for the human embryo implantation and slowing down its tubal transport…
[1] W.M. Moore “Ovulation symptoms and avoidance of conception”. Lancet, str. 588, 11 marca 1972 oraz T.W. Hilgers i współautorzy „The Peak symptom and estimated time of ovulation”. Obstetrics and Gynecology, 52:5, str. 575-582, listopad 1978.
[2] J.B. Stanford, G.L. White Jr, H. Hatasaka ”Timing intercourse to achieve pregnancy: current evidence”. Obstetrics & Gynecology, No 6, 100, str. 1333-1341, 2002.
[3] J. Rötzer z E. Rötzer „Ja i mój cykl. Od okresu pokwitania do lat przejściowych”. INER, Warszawa 2007.
[4] D.A. Grimes, A.J. Godwin, A. Rubin “Ovulation and follicular development associated with the low-dose oral contraceptives: a randomized controlled trial”. Obstetrics and Gynecology Journal No 83, str. 29-34, 1994.